
HSAG Assists Critical Access and Rural Hospitals to Reduce HAIs Using TAP Reports and Interactive Dashboards
Health Services Advisory Group (HSAG), a Centers for Medicare & Medicaid Services (CMS) Hospital Quality Improvement Contractor (HQIC), helped more than 112 critical access and rural hospitals and those serving vulnerable populations reduce Healthcare-Associated Infections (HAIs), including Catheter-associated Urinary Tract Infections (CAUTI), Clostridioides difficile Infection (CDI), Methicillin-resistant Staphylococcus aureus (MRSA), Surgical Site Infection (SSI), and Central Line-Associated Bloodstream Infections (CLABSI).
As a first step, HSAG assists hospitals with entering data into the Centers for Disease Control and Prevention (CDC) National Healthcare Safety Network (NHSN), the nation’s most widely used HAI tracking system. Once hospitals have completed their data entry, HSAG is granted permission to access their data. Using a combination of NHSN and CMS claims data, HSAG then identifies hospitals that need additional assistance to reduce HAIs.
Healthcare Safety Network (NHSN), the nation’s most widely used HAI tracking system. Once hospitals have completed their data entry, HSAG is granted permission to access their data. Using a combination of NHSN and CMS claims data, HSAG then identifies hospitals that need additional assistance to reduce HAIs.
The Targeted Assessment for Prevention (TAP) Strategy is a framework for quality improvement that uses data for action to prevent HAIs by targeting hospitals with an excess burden of infections, assessing for gaps, and implementing prevention strategies. HSAG uses this framework to produce a TAP Report that aggregates data from all of HSAG’s participating hospitals. The TAP Report ranks hospitals by the Cumulative Attributable Difference (CAD), which identifies the number of excess infections that the hospital must reduce to reach the target prevention goal. For example, if a hospital has exceeded its threshold of two infections, the CAD will indicate that the hospital is still two infections above its goal. Small hospitals often don’t think they have to reduce their infections when they can’t generate a Standardized Utilization Ratio (SUR), a summary measure used to track device use at the local or facility level over time. Therefore, coaching these facilities to use these data is critical to infection reduction.
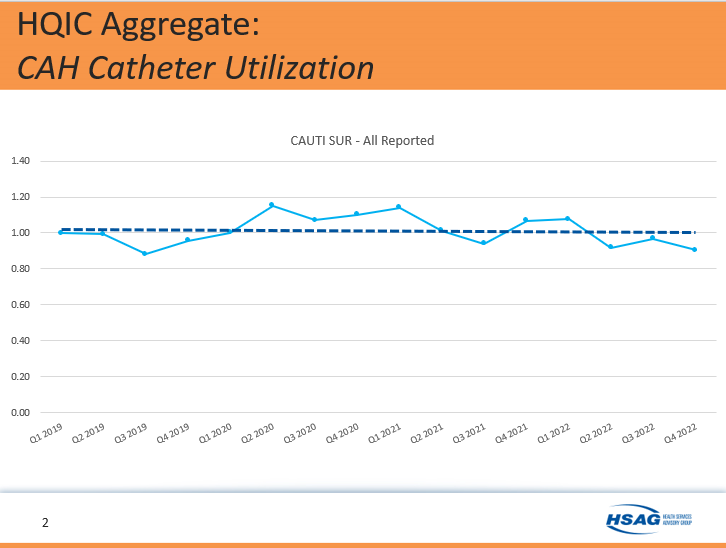
Although critical access hospitals tend not to have many infections, HSAG did observe an increase in catheter use during the COVID-19 pandemic. This is illustrated in HSAG’s HQIC Summary—CAH Catheter Utilization for CAUTI SUR from Quarter 1 2019 through Quarter 4 2022 in Graph 1 below.
Graph 1.
HSAG HQIC Dashboard
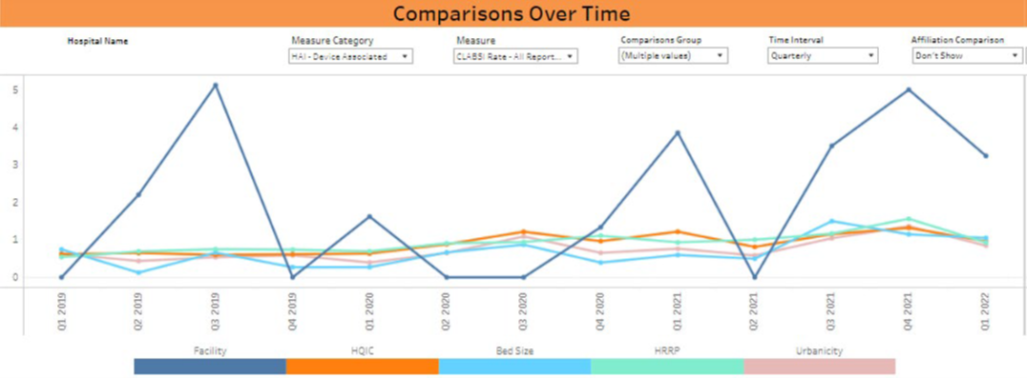
One challenge HSAG identified in its work with small hospitals is that there are no data that compare one HSAG HQIC hospital to another. To address this challenge, HSAG developed the HSAG HQIC Hospital Dashboard. The dashboard allows hospitals to develop peer groupings that create benchmark data between hospitals and generate run charts to see if their experiences are unique or similar to other hospitals across the HSAG HQIC. (See Graph 2). Run charts can be created by Measure Category, Measure, Comparison Group, Time Interval, and Affiliation Comparison.
Graph 2.
Technical Support
HSAG provides TAP education through webinars, consultive telephone calls, and emails. NHSN support is offered by assisting with creating a group and accessing, running, and interpreting TAP Reports. Providing data-driven technical support and education to hospitals about the NHSN system and how it can engage partners to help hospitals move in the right direction to eliminating HAIs has been key to HSAG HQIC’s success.
For more information, visit HSAG HQIC.
Telligen Assists Hospital to Reduce CLABSI and CAUTI Rates Using TAP Report
Telligen HQIC has seen participating hospitals reduce their CLABSI and CAUTI rate using TAP Reports. Using webinars, one-on-one meetings and learning collaboratives, Telligen teaches hospitals to use the reports to identify opportunities for improvement and how to run the reports themselves, if needed.
Following Telligen’s recent CLABSI Sprint which featured presentations on quality Improvement basics and detailed guidance on how to run and utilize TAP Reports for quality improvement, one hospital was able to gain valuable information from the TAP Report despite consistently having small denominators for the CAUTI rate measure. The hospital also used the TAP Reports to establish a goal for 2022. See the example from NHSN below.
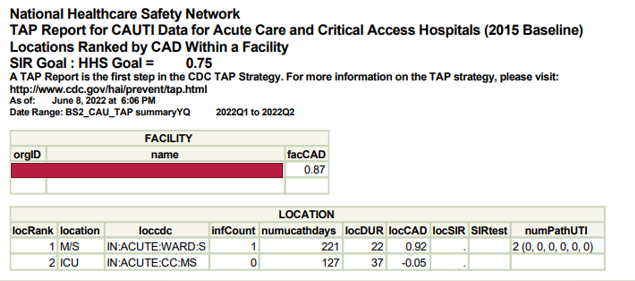
The hospital’s infection preventionist used the facility’s CAUTI Cumulative Attributable Difference (CAD) to motivate her team members to action. While the CAD is unit specific and not a comparative metric, it is a good way for small facilities to know if they have more infections than is recommended for their size and unit type. A CAD of “1” or higher is a sign that there are too many infections on the unit.
From Quarter 1 to Quarter 2 2022, the hospital showed one CAUTI in the medical-surgical nursing (Med-Surg) unit under Infection Count (infCount). A CAD above zero shows that for the size of the unit and patient days, the unit should have one (0.92 rounded up) less infection than what was reported on Med-Surg for Quarter 1. Therefore, the goal for the Med-Surg unit is to have “0” CAUTIs. Although the unit did not need to reduce by several CAUTIs, the goal of reducing by one infection was clear and realistic for the staff. The CAD for the Intensive Care Unit shows no infections and a zero CAD (-0.05 rounded to 0), therefore no decrease in infections was needed.
The infection preventionist followed up her TAP education with a review of best practices for preventing CAUTIs. Staff knowledge was validated through a quiz and a Days Since Last CAUTI poster was emailed to staff each quarter. As a result, the team had zero CAUTIs in Q2 2022 and just one CAUTI in Q3 2022. Data for Q4 2022 is pending.
For more information, visit TelligenQIConnect.com.
This material was prepared by The Bizzell Group (Bizzell), the Data Validation and Administrative (DVA) contractor, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services (HHS). Views expressed in this material do not necessarily reflect the official views or policy of CMS or HHS, and any reference to a specific product or entity herein does not constitute endorsement of that product or entity by CMS or HHS. 12SOW/Bizzell/DVA-1141-07/18/2023